10/13/2008 - Healthcare System Solutions recently attended the SECAPS (Southeastern College of Anticoagulation Providers) conference in Franklin, TN on October 10-11th, 2008.
We met a lot of great people with clinics that could greatly benefit from our INR Pro product!
The following are some highlights from the conference presenters, related to INR Pro.
Patient Self-Testing (PST)
He referred to the 4 C's for evaluating patients for self-testing:
National Patient Safety Goals for Anticoagulation: Are You Ready? As of October 1, 2008, the expectation states that pilot testing in at least one clinical unit should be under way (INR Pro can help address the following implementation expectations: A1, C4, A5, C9, C10, A11). As of January 1, 2009, all clinics should be compliant to the goals. According to Gulseth, this means clinics must evaluate their anticoagulation safety practices, show continuous improvement actions, and measure effectiveness of actions on a regular basis. They should also define what baseline history of INR results entails, and what constitutes a current INR value (i.e. if more than 24 hours, then re-test). INR Pro can work with you to upload historical data to fulfill the baseline data requirements, and will provide the system to meet all of the continuous improvement requirements.
The guidelines that are currently available are not geared towards in-patient settings, so he provided a set of guidelines for new patients that he feels works pretty well.
In addition for in-patient management, he recommends creating and implementing a patient discharge checklist for any patient on warfarin/Coumadin. It should make sure that all aspects of care have been completed, an anticoagulation order with details has been submitted, and the patient has received warfarin/Coumadin training

Dr. Mark Wurster, Ohio State University Internal Medicine
Michael Gulseth, PharmD, University of Minnesota College of Pharmacy

![]() If you would like to take advantage of these features with INR Pro, try our demo, or contact us for more information.
If you would like to take advantage of these features with INR Pro, try our demo, or contact us for more information.
Helping manage anticoagulation patients for over 21 years

INR Pro highlighted in latest issue of Group Practice Journal!
Latest Articles
INR Pro featured in medical group magazine
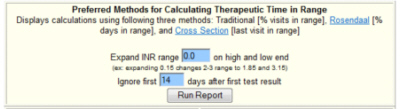
Rosendaal method for patient TTR calculations available in Excel template
New INR data reports available from your current anticoagulation system

Monitored by Site24x7
Uptime